A Plain-English Field Manual
The Menopause Guide.
The 100+ symptoms. The science your doctor skipped. The treatment decisions no one walked you through. Everything you should have been told — in one place.
"You're not broken.
You're not crazy.
And you are absolutely not alone."
If you've picked up this guide, something is probably not right. The sleep that used to come easily doesn't anymore. The body you knew for forty years feels unfamiliar. You cry at car commercials, forget the word for "refrigerator," and wake at 3 a.m. with your heart pounding for no reason at all.
You've likely been told it's stress. That it's "just aging." That you should try yoga, cut out wine, or perhaps take an antidepressant. Maybe you've started to wonder if this is simply who you are now.
It isn't. What you are experiencing has a name, a mechanism, and — most importantly — an evidence-based treatment. In the ten chapters that follow, the pieces come together. By the end, you will know exactly what is happening in your body, why, and what your options are.
— From the editors at ILSA Health
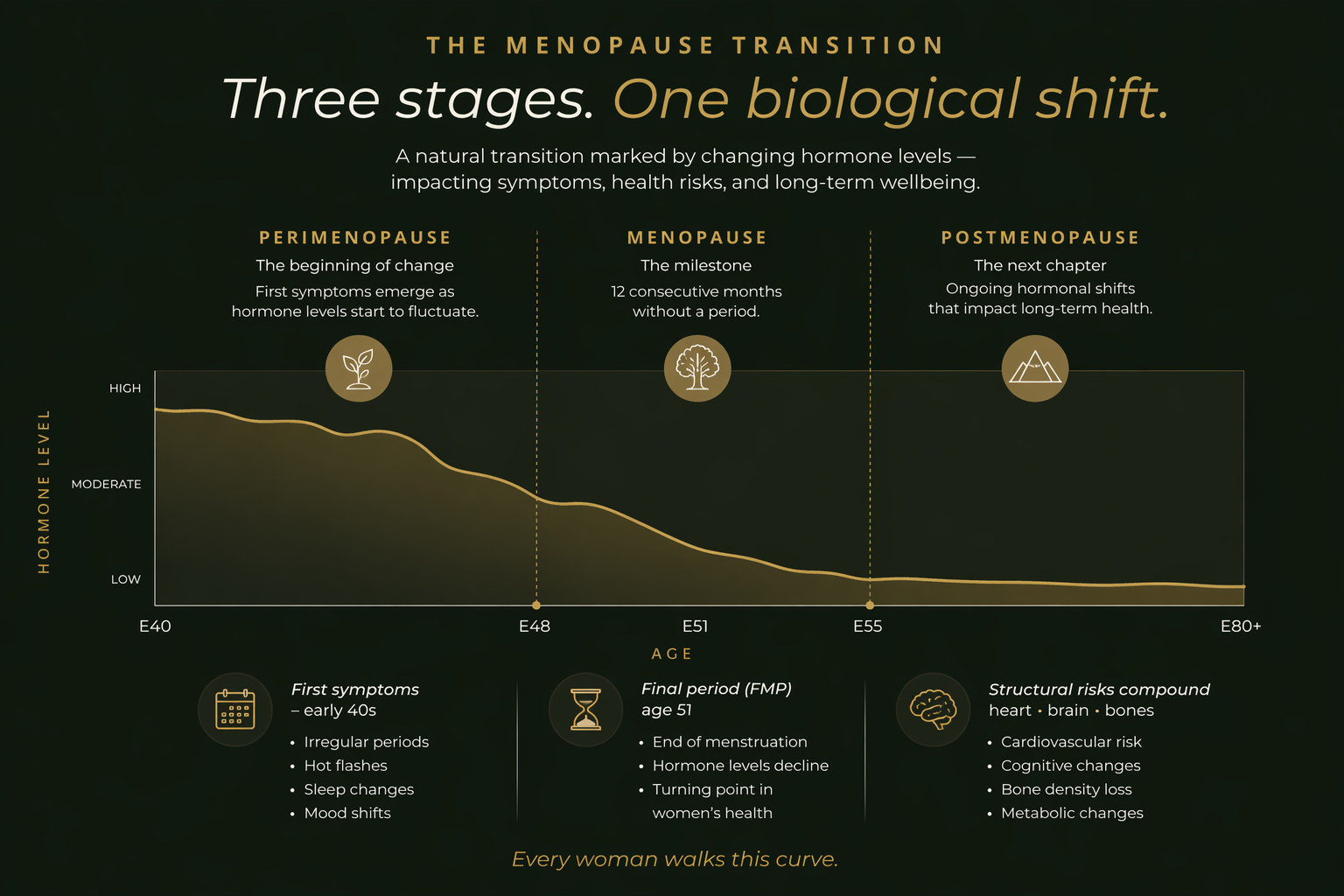
Menopause is not a moment.
It's a decade.
Most women have been taught there are two states — "having periods" and "menopausal." The truth is there are three distinct phases, each with its own hormonal signature and symptom profile.
The silent decade. Estrogen does not decline in a smooth line — it spikes and crashes, often violently, within the same week. This is the most symptomatic phase for most women, because the body is constantly readjusting to shifting hormone levels rather than a stable new baseline.
Technically a retrospective diagnosis: twelve full months with no period. By this point, the ovaries have largely stopped producing estrogen. Hormone levels have dropped to their new baseline — roughly 90% below premenopausal levels. Some perimenopausal symptoms ease. Others intensify.
The rest of life. Acute symptoms — hot flashes, sleep disruption — gradually improve for many women during the first five to ten years. But the silent structural effects of low estrogen continue to compound: bone loss, cardiovascular risk, cognitive decline, urogenital atrophy.
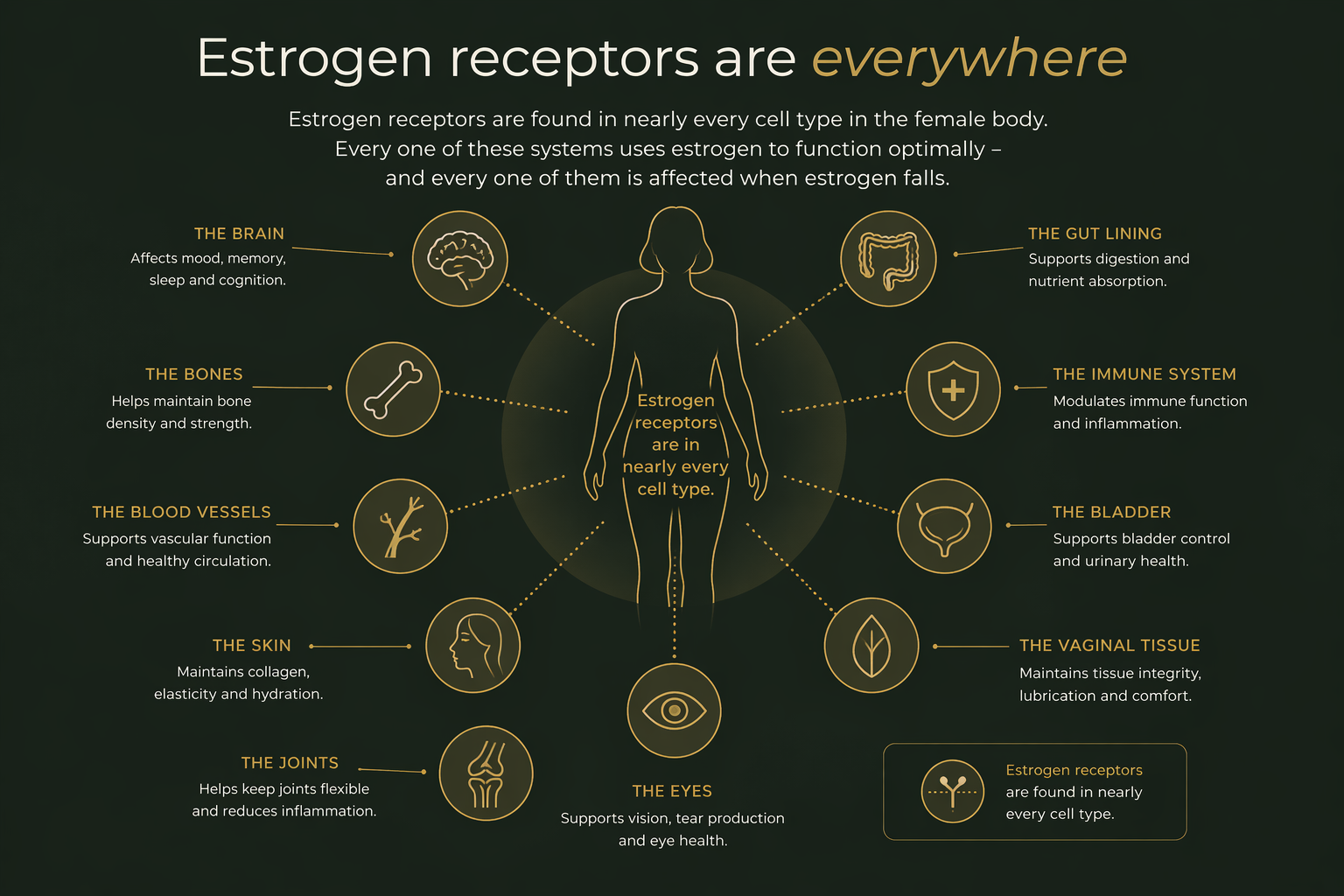
Estrogen isn't a reproductive hormone.
It's a whole-body hormone.
If you have ever wondered why menopause produces a hundred different symptoms rather than one or two, the answer is in your cells. Estrogen receptors are present in nearly every tissue of the female body. When estrogen drops, every one of these systems is affected in parallel.
100+ symptoms. Eight systems.
One underlying cause.
Most symptom lists throw everything at you in one long column. We've organized menopause's hundred-plus known symptoms by the body system they come from — so you can see the pattern instead of the noise.
Vasomotor
Sleep & Fatigue
Cognitive & Mood
Urogenital
Cardiovascular
Musculoskeletal
Skin, Hair, Eyes
Weight & Metabolism
The study that scared a generation of women off the medicine that could have helped them.
For more than two decades, a single flawed interpretation of the Women's Health Initiative scared millions of women — and their doctors — away from hormone therapy. The science has since corrected itself. Most doctors' training hasn't caught up.
"HRT causes breast cancer."
The 2002 WHI headline claimed a "26% increased risk" — a scary relative number that translated to roughly 8 additional cases per 10,000 women per year. The study used a synthetic oral estrogen-progestin combination, in women averaging 63 years old — many of whom were already a decade past menopause.
Bioidentical HRT, started in the window, is among the most beneficial medicines in modern medicine.
Reanalysis of the WHI data (and every major study since) shows that in women under 60 or within 10 years of menopause, HRT reduces all-cause mortality, protects the heart, preserves bone, and cuts dementia risk. NAMS, ACOG, and the Menopause Society now explicitly endorse it for symptomatic women in the window.
"Hormones are unnatural and risky."
The fear is often attached to the word "hormones" as if it meant something foreign. The WHI trial used conjugated equine estrogens — harvested from pregnant horse urine — paired with a synthetic progestin unlike anything your body produces.
Bioidentical estradiol is molecularly identical to the estrogen your own ovaries made for 35+ years.
It's not a new or foreign substance. It's the same molecule — delivered in a steady, measured dose. The modern preferred delivery is transdermal (patch or gel), which bypasses the liver entirely and avoids the clotting risk associated with older oral formulations.
"You should wait until symptoms are unbearable."
Many women are told — often by their own doctors — to "push through" and only consider HRT as a last resort after years of escalating symptoms. This advice unknowingly squanders the single most important variable in long-term outcomes: timing.
The earlier within the window you start, the greater the long-term protection.
Women who begin HRT in perimenopause or within 10 years of menopause see the largest benefits to bone, brain, and cardiovascular health. Starting later is still often beneficial for symptom relief — but the preventive benefits shrink the longer you wait.
Patch, gel, or tablet.
Which one is right for you?
Bioidentical estradiol is prescribed in three primary forms. Each delivers the same molecule — what differs is how it enters your bloodstream, how steady the levels are, and how forgiving the daily routine is.



From this guide to your first prescription, in three steps.
You've read the science. You know which form of estradiol your provider is most likely to consider. Here is exactly what happens when you press "Start My Free Visit" — from the first click to your first application.
The ten years that matter most.
The single biggest predictor of long-term HRT benefit is not your symptoms. It's your timing. Starting bioidentical hormone therapy in perimenopause or within ten years of your last period gives you the full cardiovascular, cognitive, and skeletal protection HRT is capable of delivering.
Outside that window, HRT is still often a powerful symptom treatment — but the preventive effects on heart and brain diminish. This is why "wait and see" is, for most women, the wrong strategy.
HRT is the lever.
Lifestyle is the foundation.
Hormone therapy is the most effective single intervention for menopausal symptoms. But it is not a substitute for the four pillars every woman in midlife should anchor into. Done together, they compound.
Sleep
Seven-plus hours, cool bedroom, consistent wake time. Avoid alcohol past 6 p.m. — it is the single biggest trigger for 3 a.m. waking in perimenopause. Magnesium glycinate before bed, blackout curtains, no phone in reach.
Strength
Lift heavy things, twice weekly, for the rest of your life. Muscle mass protects bone, sugar metabolism, and mood. Cardio alone is not enough after 40 — resistance training becomes preventive medicine.
Protein & fiber
Aim for 1g of protein per pound of lean body weight. Emphasize fiber from vegetables, berries, beans, and whole grains. Limit alcohol and ultra-processed food. Prioritize phytoestrogen-rich foods: flax, soy, lentils.
Stress & cortisol
Chronic stress elevates cortisol, which directly worsens hot flashes, sleep, and belly-fat gain. Breathwork, walks without a phone, and adaptogens like ashwagandha quiet the sympathetic nervous system in the short and long term.
The five supplements that actually help in menopause.
Supplements don't replace hormones. But a carefully chosen stack can take the edge off cortisol spikes, support sleep, protect bone and heart, and give skin back some of what estrogen used to guarantee.
Ashwagandha Plus
Adaptogenic root that lowers cortisol, calms anxiety, and supports deeper sleep. The single most useful supplement for hormonal stress in midlife.

5-HTP
Serotonin precursor for mood balance and deeper sleep. Estrogen loss disrupts serotonin signaling — 5-HTP helps restore it naturally.

Bone & Heart Support
Calcium, magnesium, vitamin K2, and D3 to protect bone density and cardiovascular health — both at risk the moment estrogen falls.

Anti-Aging Moisturizer
Peptide-rich daily moisturizer that rebuilds the moisture barrier estrogen used to maintain. For the skin you remember.

Bee Pearl
Royal jelly, bee pollen, and propolis — a potent natural source of B vitamins, amino acids, and adaptogens for daily midlife vitality.
When it's not menopause — and when to seek care in person.
Menopause causes a lot. But some symptoms are not menopause, or not only menopause. The following signs warrant in-person evaluation with your primary care provider, a specialist, or — in urgent cases — emergency care. Do not wait on a telehealth intake for these.
If you are in crisis, the 988 Suicide & Crisis Lifeline is available 24/7 — call or text 988. This guide is educational and is not a substitute for medical advice from a licensed clinician who knows your full history.
The questions most women don't get answered.
Every term in one place.
Medical language makes menopause harder than it already is. Here is the vocabulary you will hear from a provider, in ordinary English.
The version of you you remember
She's still in there.
And she's tired of waiting.
You've read the guide. You know what's happening now. The next step is a ten-minute visit — the same science you just read, translated into a prescription written for your life. No clinic waiting rooms. No gatekeeping. Just care from a licensed provider through ILSA.
Start My Free VisitILSA Health is a telehealth platform that connects patients with independent U.S.-licensed healthcare providers; it is not a medical group and does not itself prescribe medication. Bioidentical estradiol is available by prescription only and requires licensed provider evaluation. Individual results vary. Compounded medications are not FDA-approved. All prescriptions are fulfilled by independent U.S.-licensed pharmacies. Completion of an assessment does not guarantee approval or create a physician–patient relationship. Testimonials reflect individual experiences and are not a guarantee of results. Hormone therapy is not appropriate for all women. Consult a licensed provider regarding contraindications. This guide is educational and is not a substitute for medical advice.